Image


This article is updated with a table with more details on treatment of EHV-1 at the bottom of the article.
In light of the current outbreak of Equine Herpes Virus-1 (EHV-1) the European College of Equine Internal Medicine has decided to provide the following guidelines available to anyone dealing with horses returning from Valencia/Spain or as general guidelines to deal with such outbreaks. Horse owners should seek advice from their veterinarian but may wish to quote these guidelines.
EHV-1 is a common virus that affects horses worldwide and can cause mild respiratory disease, and on occasion, serious complications of neurological gait deficits. Clinical signs may include nasal discharge, cough, a rectal temperature greater than 38.3°C/101.5°F, enlarged submandibular lymph nodes and oedema of the limbs and/or ventral abdomen. Neurological signs can be any of urinary/faecal incontinence, penile prolapse, weak tail, being unsteady on its feet or even being unable to stand, which may deteriorate requiring euthanasia. Owners of horses suffering from any on these signs or in contact with a horse with any of these signs please contact your veterinarian immediately.
All horses returning home from Valencia/Spain or from a show where horses from Valencia were present should undergo the following protocol:
Lutz Göhring, Karsten Feige, Marianne Sloet, Dominique De Clercq, Vinzenz Gerber, Orsolya Korbacska-Kutasi, Ignacio Corradini, Fernando Malalana, Ruth Morgan, Lisa Katz, René Van den Hoven, Marco Duz, Jessika-M. Cavalleri, Anne Couroucé
Once biosecurity/quarantine guidelines have been followed, there are numerous medical options for treatment of Equine Herpesvirus-1 (EHV-1) positive horses with and without clinical signs of Equine Herpesvirus Myeloencephalopathy (EHM). If a horse begins to show clinical signs of EHM, it is important to consider that intensive and committed nursing care plays a pivotal role in the management of these cases. This may include provision of soft bedding and helmets to protect the horse from head trauma, the use of indwelling urinary catheters and manual evacuation of the rectum and assisting the horse to stand (using slings) if possible. If the horse is unable to stand the horse should be maintained in sternal recumbency, and rolled to different sides every 2-4 hours. Monitoring and maintaining hydration is vitally important.
Table 2: Commonly used drugs for EHV-1 positive horses, both with and without clinical signs of EHM.
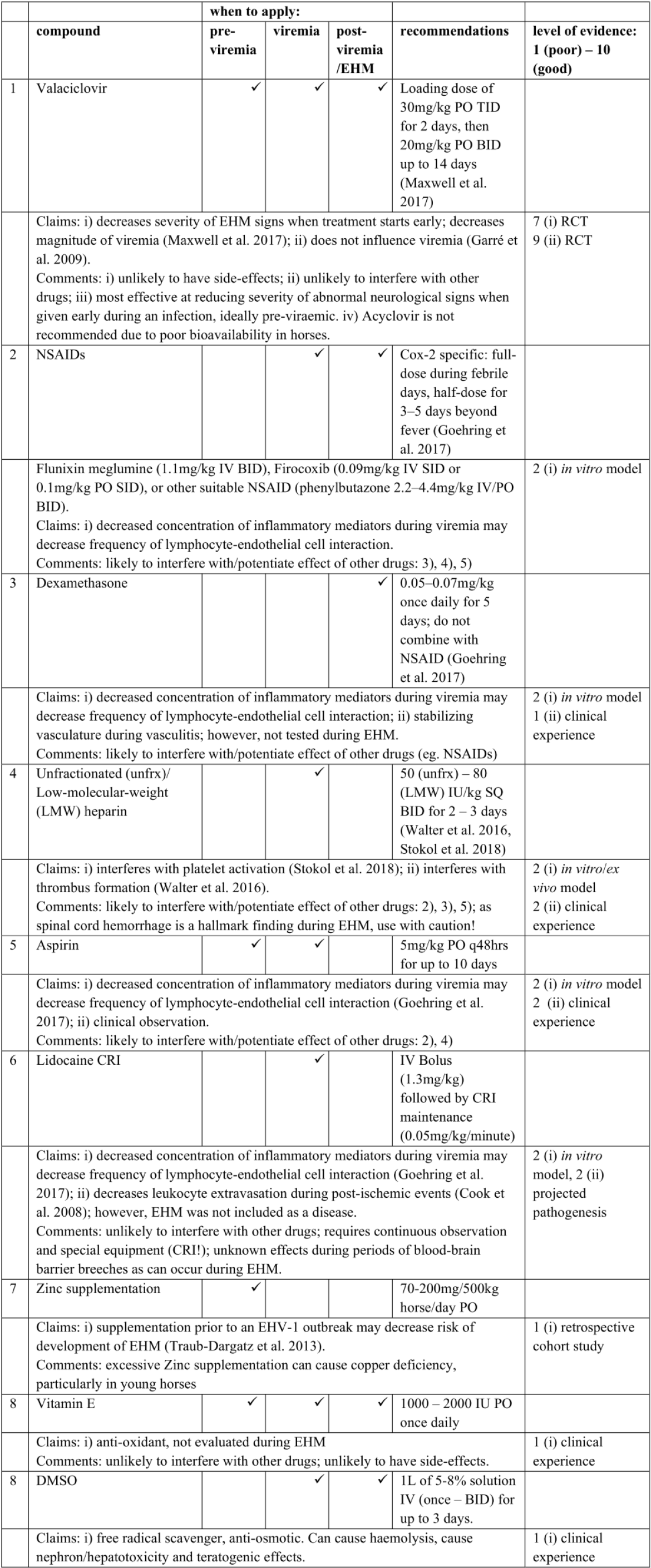
RCT: Randomised Control Trial; CRI: Constant Rate Infusion; DMSO: Dymethyl sulphoxide;
For further advice please check www.eceim.info/diplomats to find a Recognised Equine Internal Medicine Specialist closest to you.
Lutz Göhring, Karsten Feige, Marianne Sloet, Dominique De Clercq, Vinzenz Gerber, Orsolya Korbacska-Kutasi, Marco Duz, Jessika-M. Cavalleri, Anne Couroucé
Cook VL et al. (2008) Attenuation of ischaemic injury in the equine jejunum by administration of systemic lidocaine. Eq Vet J. 40:353-357
Garré B et al. (2009) Evaluation of orally administered valacyclovir in experimentally EHV1-infected ponies. Vet Microbiol. 135:214-221
Göhring L et al. (2017) Anti‐inflammatory drugs decrease infection of brain endothelial cells with EHV‐1 in vitro. Eq Vet J. 49(5):629-636
Maxwell LK et al. (2017) Efficacy of the early administration of valacyclovir hydrochloride for the treatment of neuropathogenic equine herpesvirus type-1 infection in horses. Am J Vet Res. 78(10):1126-1139
Stokol T et al. (2016) Unfractionated and Low-Molecular-Weight Heparin and the Phosphodiesterase Inhibitors, IBMX and Cilostazol, Block Ex Vivo Equid Herpesvirus Type-1-Induced Platelet Activation. Front Vet Sci. 17:99
Traub-Dargatz et al. (2013) Case-Control Study of a Multistate Equine Herpesvirus Myeloencephalopathy Outbreak. J Vet Int Med. 27(2):339-346
Walter J, et al. (2016) Prevention of equine herpesvirus myeloencephalopathy - Is heparin a novel option? A case report. Tierarztl Prax Ausg G Grosstiere Nutztiere. 44:313-317